Surgery may be suggested if all else fails. Several types of procedures are useful in treating this condition.
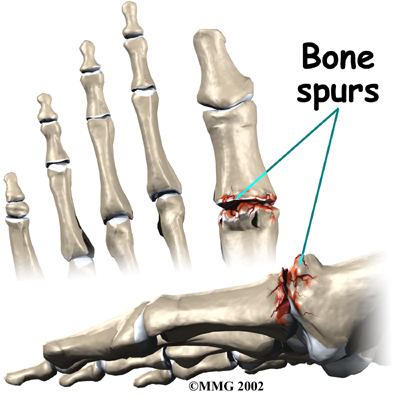
In some cases bone spurs that form on the top of the joint can bump together when the big toe bends upward, or extends. This causes a problem when walking because the big toe needs to bend upward when the foot is behind the body, in order to take the next step. The constant irritation when the bone spurs bump together leads to pain and difficulty walking.
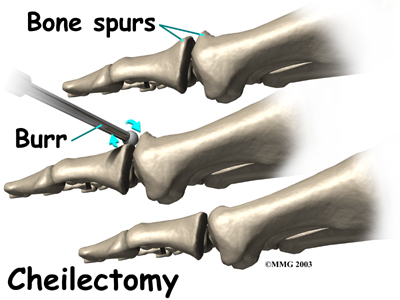
A cheilectomy is a procedure to remove the bone spurs at the top of the joint so that they don't bump together when the toe extends. This allows the toe to bend better and reduces the amount of pain while walking. To perform a cheilectomy, an incision is made along the top of the joint. The bone spurs that are blocking the joint from extending are identified and removed from both the bones that make up the joint. A little extra bone may be taken off to ensure that nothing rubs when the hallux is raised. The skin is closed and allowed to heal.
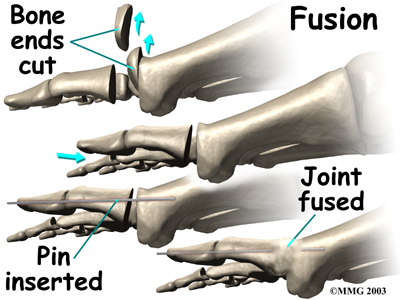
Many surgeons prefer arthrodesis, or fusion, of the MTP joint to relieve the pain. To fuse a joint means to encourage the two bones that form a joint to grow together and become one bone. To perform a fusion, an incision is made into the MTP joint. The joint surfaces are removed. The two surfaces are then fixed with either a metal pin or screw, with the toe turned slightly upward to allow for walking. The bones are then allowed to fuse. The fusion usually takes about three months to become solid.This results in a joint that no longer moves. Wearing a rocker-soled shoe is usually necessary following a fusion to improve your gait.
Some surgeons prefer replacing the joint with an artificial joint, similar to what is done in the knee or hip, only much smaller. Replacing the joint with an artificial joint is usually recommended for moderately involved joints. (Many surgeons, however, believe that arthrodesis or fusion still produces better results for patients with severe hallux rigidus.)
In this procedure, one of the joint surfaces is removed and replaced with a plastic or metal surface. This procedure may relieve the pain and preserve the joint motion. The major drawback to this procedure is that the artificial joint will probably not last a lifetime and will require more operations later if it begins to fail.
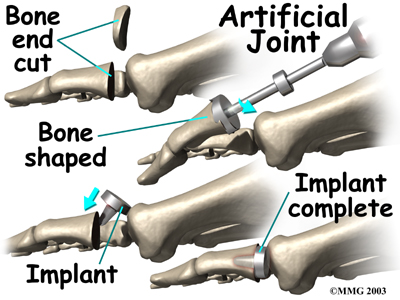
To perform an artificial joint replacement, an incision is first made on the top of the big toe over the MTP joint. Once the joint is surgically entered, the arthritic joint surface of the proximal phalanx (the first bone of the big toe) is removed. The hollow marrow area of the proximal phalanx is prepared with special instruments so that the artificial joint surface will fit snugly into the bone. Different sized implants are tried, and the toe is moved through a range of motion to help determine if the fit is proper.
Once the surgeon is satisfied that everything fits, the artificial joint surface is implanted. The joint capsule and skin incision are then closed with small stitches.
There are actually several different ways to accomplish a joint replacement for hallux rigidus. A total joint replacement removes and replaces both sides of the joint. This type of procedure requires a conical stem that sits down inside the toe bones on either side of the joint. The implants can be made of ceramic, titanium, cobalt-chrome, or titanium combined with polyethylene (plastic) parts.
Metatarsal hemiarthroplasty replaces just one side of the joint; the one between the bone closest to the middle part of the foot (metatarsal) and the middle phalangeal bone. Limited studies have been done using this approach but patient satisfaction is reportedly high with few implant failures or need for revision surgery.
There are other surgical procedures that are slight variations of these three approaches. For example, cheilectomy may be combined with a phalangeal osteotomy. With the osteotomy the surgeon removes a wedge-shaped piece of bone from the middle toe bone in order to take pressure off the joint. Some patients can be successfully treated with just the osteotomy procedure.
Another alternative approach (more for the younger patient) is the interpositional arthroplasty. In this procedure, the surgeon removes the base of the toe bone (phalange) and places a "spacer" in the hole left. The spacer is made up of a rolled up piece of tendon. The surgeon may have to release the tendon that inserts into the base of the phalange for this to work best. This decision is made at the time of the surgery.
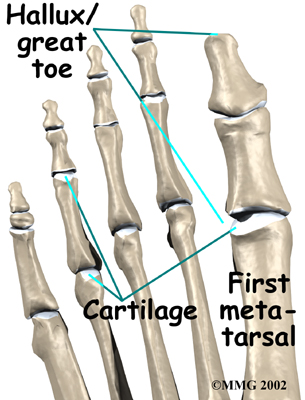
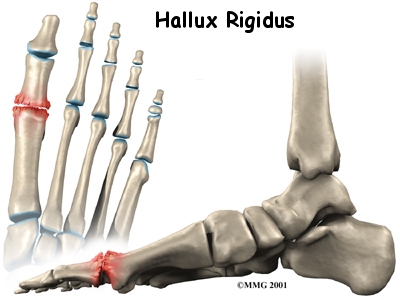 Hallux rigidus is a degenerative type of arthritis that affects the large joint at the base of the big toe (sometimes called the great toe). Degenerative arthritis results from wear and tear on the joint surface over time. The condition may follow an injury to the joint or, in some cases, may arise without a well-defined injury.
Hallux rigidus is a degenerative type of arthritis that affects the large joint at the base of the big toe (sometimes called the great toe). Degenerative arthritis results from wear and tear on the joint surface over time. The condition may follow an injury to the joint or, in some cases, may arise without a well-defined injury.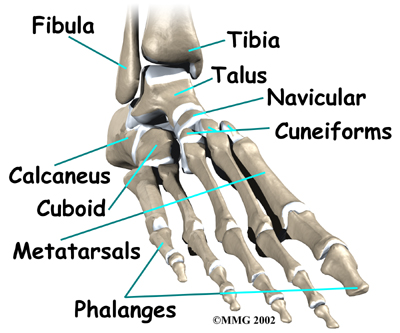


 (403) 679-7179
(403) 679-7179  concierge@one-wellness.ca
concierge@one-wellness.ca 

