What should I expect during my rehabilitation period?
As mentioned above, you will wear a cast on your arm and hand for about six weeks to give the fusion time to heal. When the cast is removed, you may have stiffness or pain in the joints closest to the fused joint or pain around the surgical incision. physiotherapy at One Wellness will help relieve your pain and decrease the stiffness in the surrounding joints.
In order to decrease pain we may use modalities such as heat, ice, or electrical current.
These will assist with managing pain and any ongoing swelling you have around the surgical site, anywhere along the arm, or into the hand. Massage to these areas may also be done in order to improve circulation and assist with easing any discomfort. Some of the muscles of the neck may also be painful from having the arm in a cast for an extended period. These muscles may also benefit from massage treatment, which will make movement of your entire surgical side easier.
The next part of our treatment will focus on regaining the range of motion, strength, and dexterity in the joints on either side of your fused finger as well as your other fingers, wrist, hand, elbow, and even shoulder. As the motion of your fused joint will be permanently lost, it is of paramount importance to maintain the range of motion, strength, and dexterity in the joints surrounding the fusion in order to be able to continue to use your hand functionally. Your physiotherapist at One Wellness will prescribe a series of range of motion and strengthening exercises that you will practice in the clinic and also learn to do as part of your home exercise program. These exercises may include the use of rehabilitation equipment such as mini pulleys, putty, elastics or balls for strengthening and gripping resistance. In addition to strengthening your grip we will educate you on ways to grip and support items in order to do your daily tasks by compensating for your surgical finger but without putting too much stress on your healing fusion or the other joints.
If necessary, your physiotherapist will mobilize the joints above and below your fused joint or any other joint in the area that is stiff and impeding movement of your hand and limb. This hands-on technique encourages the stiff joints to move gradually into their normal range of motion.
Being able to move your hand and finger so that you can complete your work tasks and daily activities is the goal for our therapy at One Wellness. Maximizing dexterity can greatly improve the functional use of your hand. For this reason, we will also incorporate functional activities like picking up items from a table or twisting items into place using your surgical hand. These functional activities encourage the joints and the muscles of the hand and arm to work in unison, which is critical to maximizing the use of your overall upper limb. Exercises where weight is put through your fused joint, such as pressing the pad of your finger into something, will also be added when appropriate to encourage the fusion to tolerate weight in a controlled fashion.
When you are well underway, regular visits to One Wellness will end. Your therapist will continue to be a resource, but you will be in charge of doing your exercises as part of an ongoing home program. Generally, the majority of your gains from physiotherapy will occur within the first 1-2 months after the joint is fused. Since the fused joint does not move and therefore does not need any therapy to gain range of motion itself, improvements with therapy at One Wellnessafter a finger joint fusion are noticed very quickly.
Generally the physiotherapy we provide at One Wellness after finger joint fusion occurs without any complications. If, however, during rehabilitation your pain continues longer than it should or therapy is not progressing as your physiotherapist would expect, we will ask you to follow-up with your surgeon to confirm that the joint fusion is tolerating the rehabilitation well and to ensure that there are no hardware issues that may be impeding your recovery.
One Wellness provides services for physiotherapy in Canmore.
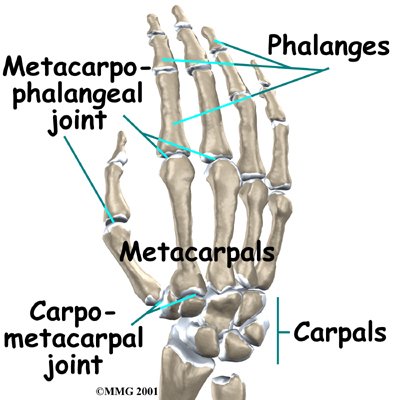 What parts of the finger are involved?
What parts of the finger are involved?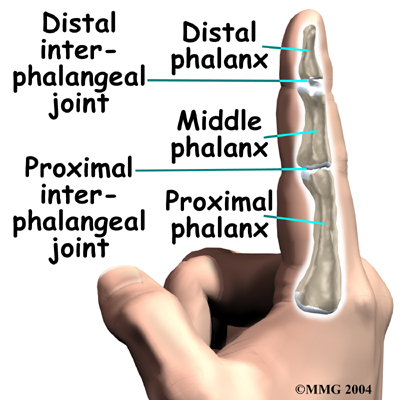
 Surgery can last up to 90 minutes. Surgery may be done using a general anesthetic, which puts you completely to sleep, or a local anesthetic, which numbs only the hand. With a local anesthetic you may be awake during the surgery, but you won't be able to see the surgery.
Surgery can last up to 90 minutes. Surgery may be done using a general anesthetic, which puts you completely to sleep, or a local anesthetic, which numbs only the hand. With a local anesthetic you may be awake during the surgery, but you won't be able to see the surgery.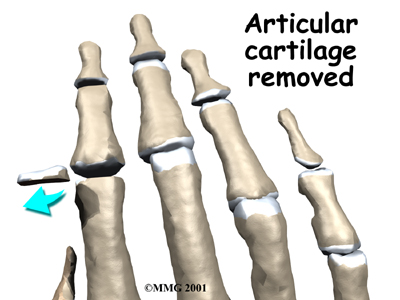

 (403) 679-7179
(403) 679-7179  concierge@one-wellness.ca
concierge@one-wellness.ca 

