What might go wrong?
Complications after a hip fracture are sometimes the result of being immobilized in bed. These may include pneumonia, bed sores, mental confusion, and blood clots (deep venous thrombosis).
Related Document: One Wellness Guide to Hip Fracture
Complications that can result from the compression fixation surgery itself include:
- anesthesia complications
- infection
- thrombophlebitis (DVT)
- nerve or blood vessel injury
- nonunion of the bones
This is not intended to be a complete list of possible complications.
Anesthesia Complications
Most surgical procedures require that some type of anesthesia be done before surgery. A very small number of patients have problems with anesthesia. These problems can be reactions to the drugs used, problems related to other medical complications, and problems due to the anesthesia. Be sure to discuss the risks and your concerns with your anesthesiologist.
Infection
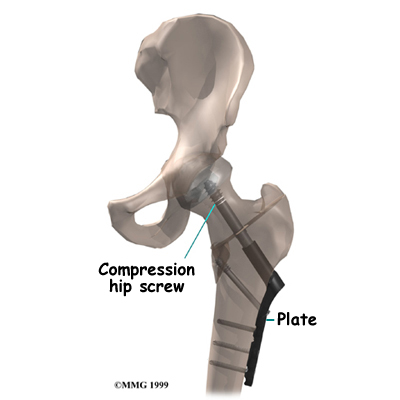
Any surgery carries the risk of infection. You will probably be given antibiotics before the procedure to reduce the risk. If you get an infection, you will need more antibiotics. If the areas around the metal screws or plate become infected, you may need surgery to drain the infection.
Thrombophlebitis (Blood Clots)
Thrombophlebitis, sometimes called deep venous thrombosis (DVT), can occur after any operation, but it is more likely to occur following surgery on the hip, pelvis, or knee. DVT occurs when the blood in the large veins of the leg forms blood clots. This may cause the leg to swell and become warm to the touch and painful. If the blood clots in the veins break apart, they can travel to the lung, where they lodge in the capillaries and cut off the blood supply to a portion of the lung. This is called a pulmonary embolism. (Pulmonary means lung, and embolism refers to a fragment of something traveling through the vascular system.) Most surgeons take preventing DVT very seriously. There are many ways to reduce the risk of DVT, but probably the most effective is getting you moving as soon as possible. Two other commonly used preventative measures include
- pressure stockings to keep the blood in the legs moving
- medications that thin the blood and prevent blood clots from forming
Nerve or Blood Vessel Injury
Several nerves and blood vessels travel in the area where the surgery is performed. It is possible to injure either the nerves or the blood vessels during surgery, but this is extremely unlikely during this type of procedure. Nerve problems may be temporary if the nerves have been stretched by retractors holding them out of the way. It is rare to have permanent injury to either the nerves or the blood vessels, but it is possible.
Nonunion
Sometimes the bones do not bond together as planned. This is called a nonunion, or pseudarthrosis. This condition requires another operation to add more fixation or to replace the head of the femur, a procedure called hemiarthroplasty.
Related Document: One Wellness Guide to Hemiarthroplasty of the Hip
After Surgery
What happens after the operation?
After surgery, your hip will be covered with a padded dressing. If your surgeon used a general anesthesia, a nurse or respiratory therapist will guide you in a series of breathing exercises. You'll use an incentive spirometer to improve breathing and avoid possible problems with pneumonia.
A physiotherapist will direct your recovery after surgery. You'll be encouraged to move from your hospital bed to a chair several times the first day after surgery. You'll be encouraged to begin getting up and walking with your crutches or walker, but you may need to keep from placing too much weight on your foot while you stand or walk. You'll be ready to go home when you can move about safely with your walker or crutches, you are able to do your exercises, and your caregiver has made all the needed preparations for you at home.
You should keep the dressing on your hip until you return to the surgeon. Avoid getting the stitches wet. Your stitches will be removed 10 to 14 days after surgery. Remember to support your outer hip with a pillow when you sit or recline.

 (403) 679-7179
(403) 679-7179  concierge@one-wellness.ca
concierge@one-wellness.ca 

