What should I expect during my rehabilitation after leaving the hospital?
After you are discharged from the hospital, you should continue your home rehabilitation program. If needed, a therapist may see you in your home for a few treatments, but this is generally only until you are able to safely get out of your home. Once you are independent enough to attend physiotherapy outside of the home, even if someone else needs to drive you, you should begin treatment at One Wellness to continue your rehabilitation. The most important part of your rehabilitation after a hip hemiarthroplasty will be the exercises that you do independently at home, however, by attending One Wellness for physiotherapy we will be able to ensure that you are doing your exercises well, ensure you are doing the correct exercises for your level of healing, advance your exercises as you improve, and ensure that there are no factors in your individual case that will impede your recover or your return to function.
If you are still using a walker or crutches by the time we first see you at One Wellness, your physiotherapist will ensure you are using them safely, properly, and confidently while abiding by your weight bearing restrictions. We will also ensure that you can safely use crutches on stairs. If you are no longer using a walking aid, or once you no longer need one, your physiotherapist will focus on normal gait re-education so you are putting only the necessary forces through the surgical side with each step, and are not compensating in any way. Until you are able to walk without a significant limp, we recommend that you continue to use a walking aid, such as your crutches, or a cane/stick. Improper gait can lead to a host of other pains in the knee, hip and back so it is prudent to use a walking aid until virtually normal walking can be achieved. Your One Wellness physiotherapist will advise you regarding the appropriate time for you to be walking without any walking aid at all.
As mentioned above, a hip hemiarthroplasty is at risk of dislocating if it is forced into certain motions, so the hip precautions you have been taught must be strictly respected, particularly in the early stages after surgery, until the incision heals and strength is regained in the muscles around the hip and in the leg. At your first appointment your physiotherapist will again discuss the hip precautions pertaining to your surgical procedure. The length of time that hip precautions should be abided by varies in opinion. Many surgeons suggest 12 weeks, however, other surgeons or health care professionals recommend much longer, even up to 1-2 years or forever, if possible! How long you must abide by your hip precautions depends on a number of factors. Certainly 12 weeks minimum is a must. Other factors affecting the length of time include: your surgeon’s protocol and recommendation based on your specific case, your muscle strength, your muscular control of the hip, your risk of falling, if you are obese, if you are very thin with little muscular support, and how active or inactive you are or want to be. Your physiotherapist at One Wellness will be able to discuss your individual situation regarding hip precautions.
During your first few appointments at One Wellness your physiotherapist will focus on relieving any pain and/or inflammation you may still have from the surgical procedure. They may use modalities such as ice, heat, ultrasound, or electrical current to assist with decreasing any pain or swelling you have around the surgical site or anywhere down the extremity. In addition, your physiotherapist may massage your hip, back, leg or ankle to improve circulation and help decrease your pain.
The next part of our treatment will focus on regaining the range of motion in your hip. Your physiotherapist at One Wellness will prescribe a series of stretching exercises that you will practice in the clinic and also add to your home exercise program. Some of these exercises may be similar to the exercises that you learned in the hospital and that you have already been doing at home. Many of the home exercises will have become too simple for you by this stage of your rehabilitation so your therapist will ensure that you are doing the most advanced exercises for your stage of recovery in order to ensure you progress as quickly as possible. Hip precautions will need to be strictly abided by in all of your exercises so it is best not to add any exercises into your program independently, but rather to allow your therapist to shape your individual program as they see fit for your current ability.
Range of motion in the hip generally comes back very quickly after a hemiarthoplasty. You may experience a small amount of discomfort at the end ranges of motion initially, but despite this it is important to perform the range of motion exercises as prescribed because moving the joint also helps to diminish the swelling, get fresh blood to the healing areas, and provides nutrition to the joint. Only mild discomfort, however, is permissible. Any sharp or moderate discomfort should be heeded. An exercise bike at this stage of recovery can be very useful, however you must still respect your hip precautions while using the bike, therefore the advice of your therapist regarding bike set up is crucial the first few times you attempt it.
If necessary, and as time and healing allows, your physiotherapist may mobilize your hip joint. This hands-on technique encourages the hip to move gradually into its normal range of motion. Mobilization of the hip may be combined with assisted stretching of any tight muscles around the surgical site.
Your therapist will also review and advance your strengthening exercises. Again, as you progress you will outgrow the strengthening exercises that were given to you in the hospital so it is important that your physiotherapist at One Wellness advances your exercises to suit your level of progress. These exercises will focus on the muscles of your hip and thigh but will also include some exercises for your back and core area as they play a large supporting role for your hips. Exercises that involve the entire lower limb, such as squats (on both legs at the same time or just one leg,) will also be given.
Exercises that work the muscles while in standing most effectively assist with daily activities such as walking and stair climbing. Other exercises in sitting or lying, however may also be prescribed. Exercises in these positions can be excellent in allowing you to target specific muscles around the hip, such as the gluteals, without causing you any discomfort from too much body weight being on the hip. Your therapist may use an electrical muscle stimulator to assist your muscles in contracting as you do your exercises; this will help you to more rapidly gain your strength back. Exercises may also include the use of exercise bands or weights to provide some added resistance for your hip and lower extremity. If you have access to a pool, your therapist may suggest you go to the pool to do your exercises. As mentioned above, the buoyancy and hydrostatic properties of the water along with the warmth of the water (provided it is a heated pool) can assist greatly in providing comfort to the hip joint and often allows your exercises to be done more easily and with less discomfort.
As a result of any injury or surgery, the receptors in your joints and ligaments that assist with balance and proprioception (the ability to know where your body is without looking at it) decline in function. A period of immobility and reduced weight bearing will add to this decline. When balance and proprioception is diminished, your joints and your limb as a whole will not function as efficiently and the decline may contribute to further injury in the future. Once you are able to put full weight onto your surgical side a final component of our treatment at One Wellness will be to prescribe exercises for you to regain this balance and proprioception. These exercises might include activities such as standing on one foot or balancing on an unstable surface such as a soft mat, or a soft plastic disc.
Proprioceptive exercises are important for all patients who have had surgery but they are particularly important for patients who have had a hip hemiarthroplasty because often the reason for the surgery was due to a fracture of the hip resulting from a fall. By improving one’s proprioception, you can decrease your chances of another fall, which may result in damage to your surgical hip, or worse yet, a fracture of the other hip or another bone in your body.
During all of your exercises your physiotherapist at One Wellness will pay particular attention to your exercise technique to ensure that you are not using any compensatory patterns or are developing bad habits in regards to how you use your hip and lower extremity. If you do not pay close attention to how you use your joint and limb post-surgically inefficient patterns can quickly occur and compensatory pain will develop either in your hip, back, or another joint. The acetabulum of the hip can also begin to quickly wear down, leading to the need for it to also be replaced, if your exercise technique or walking pattern is not pristine. Your physiotherapist at One Wellness will be crucial for providing you with feedback regarding correcting these patterns and developing new, efficient patterns during your daily activities.
As your range of motion, strength, and proprioception improve, your therapist will advance your exercises to ensure your rehabilitation is progressing as quickly as your body allows, and to incorporate exercises that simulate your specific everyday activities of daily living and any recreational activities that you may want to return to. Many patients undergoing this surgery are older, and are not still regularly active. However, there are also younger patients for whom this surgery is required. For these younger patients unfortunately, heavy sports that require running, jumping, quick stopping and starting, and cutting are discouraged. Patients may also need to consider alternate jobs to avoid work activities that require heavy demands of lifting, crawling, and climbing. Your surgeon will advise you which activities in your case are not at all permissible or are discouraged.
Your physiotherapist at One Wellness goal is to help you maximize range of motion, strength and proprioception, as well as walk normally, and improve your ability to do your activities. When you are well under way, regular visits to our clinic will end. Your physiotherapist will continue to be a resource, but you will be in charge of doing your exercises as part of an ongoing home program.
Generally the rehabilitation after a hemiarthroplasty responds very well to the physiotherapy we provide at One Wellness. If for some reason, however, your pain continues longer than it should or your therapy is not progressing as your physiotherapist would expect, we will ask you to follow-up with your surgeon to confirm that the hip is tolerating the rehabilitation well and ensure that there are no complications that may be impeding your recovery.
One Wellness provides services for physiotherapy in Canmore.
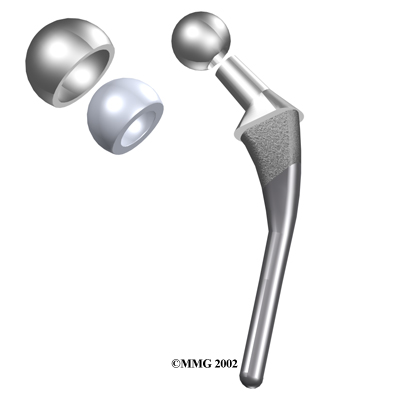
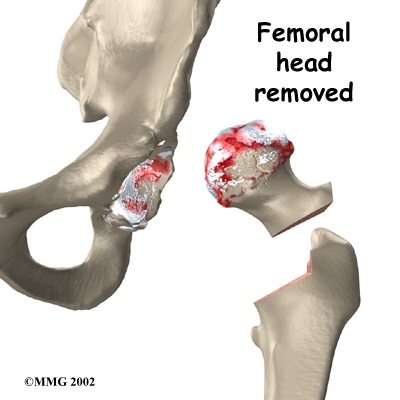
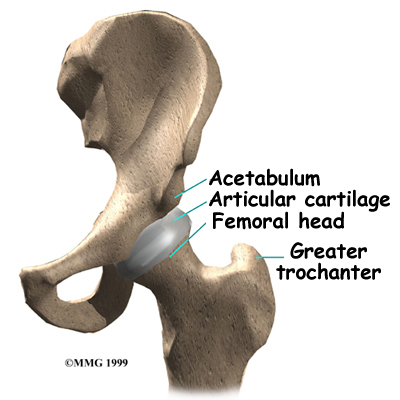 The hip joint is one of the true ball-and-socket joints of the body (the shoulder is the other.) The hip socket is called the acetabulum and forms a deep cup that surrounds the ball of the upper thighbone (femur,) known as the femoral head. The thick muscles of the buttock at the back, and the thick muscles of the thigh in the front surround the hip joint.
The hip joint is one of the true ball-and-socket joints of the body (the shoulder is the other.) The hip socket is called the acetabulum and forms a deep cup that surrounds the ball of the upper thighbone (femur,) known as the femoral head. The thick muscles of the buttock at the back, and the thick muscles of the thigh in the front surround the hip joint.

 (403) 679-7179
(403) 679-7179  concierge@one-wellness.ca
concierge@one-wellness.ca 

