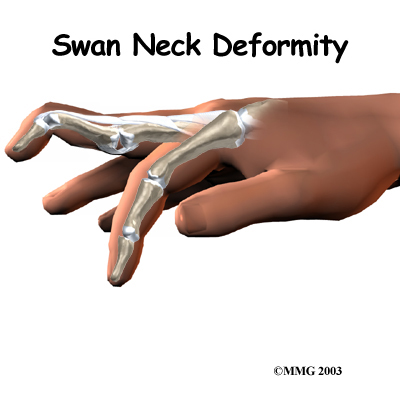
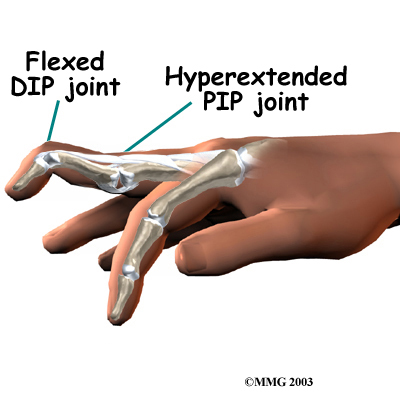
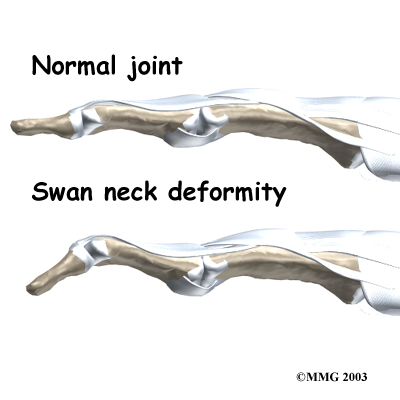
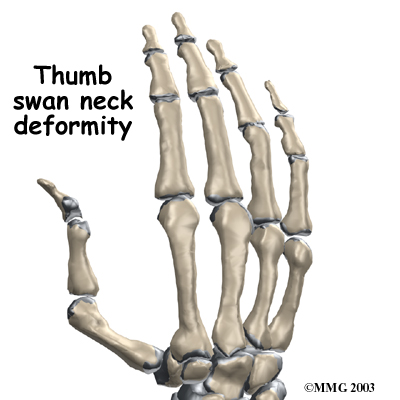
What can be done for a swan neck deformity of the finger?
Treatment for swan neck deformity can be nonsurgical or surgical. The approach used depends on whether the PIP joint is flexible or stiff.
Non-surgical Rehabilitation
Successful nonsurgical treatment is based on restoring balance in the structures of the hand and fingers. The PIP joint must be supple (not stiff). Aligning the PIP joint and preventing hyperextension should help restore DIP extension. If it doesn't, surgery may be needed.
 When you begin your One Wellness program, our physiotherapist will address the imbalances that have formed the swan neck deformity. We will use stretching, massage, and joint mobilization to try and restore finger alignment and function. Special forms of stretching may help reduce tightness in the intrinsic muscles of the hand and fingers. Our physiotherapistt will also have you perform strengthening exercises to help with alignment and function of the hand and fingers.
When you begin your One Wellness program, our physiotherapist will address the imbalances that have formed the swan neck deformity. We will use stretching, massage, and joint mobilization to try and restore finger alignment and function. Special forms of stretching may help reduce tightness in the intrinsic muscles of the hand and fingers. Our physiotherapistt will also have you perform strengthening exercises to help with alignment and function of the hand and fingers.
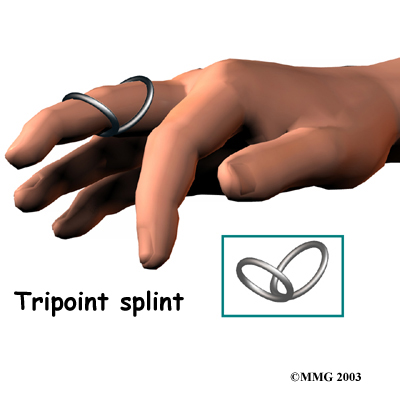
Our physiotherapist may have you wear a special splint to keep the PIP joint lined up, protect the joint from hyperextending, and still allow the PIP joint to bend. Newer styles are shaped like and are available in stainless steel, sterling silver, or gold. This approach works best for mild cases of swan neck deformity in which the PIP joint is supple.
Splinting and a rigorous physiotherapy program are usually not successful in altering the imbalance responsible for the deformity. However, many hand surgeons advise trying about six weeks with the splint and exercise to improve PIP joint mobility before performing surgery.
The goal of our nonsurgical treatment is to get your finger joints, tendons, and muscles in balance. Although the rate of recovery is different for each patient, if nonsurgical treatment is successful, you may see improvement in eight to 12 weeks.
Post-surgical Rehabilitation
You'll wear a splint or brace after surgery. A protective finger splint holds and protects the joint and is used for at least three weeks after surgery. Physiotherapy or occupational therapy treatments, such as those offered by One Wellness usually start three to six weeks after surgery.
Although each patient recovers at a different rate, it is likely that you will need to attend physiotherapy sessions for three to four months, and you should expect full recovery to take up to six months. Our first few physiotherapy treatments will focus on controlling the pain and swelling from surgery. Then our physiotherapist will have you begin doing gentle range-of-motion exercise, followed by a program of strengthening exercises starting eight to 10 weeks after surgery.
At One Wellness, our goal is to help speed your recovery so that you can more quickly return to your everyday activities. When your recovery is well under way, regular visits to our office will end. We will continue to be a resource, but you will be in charge of doing your exercises as part of an ongoing home program.
One Wellness provides services for physiotherapy in Canmore.
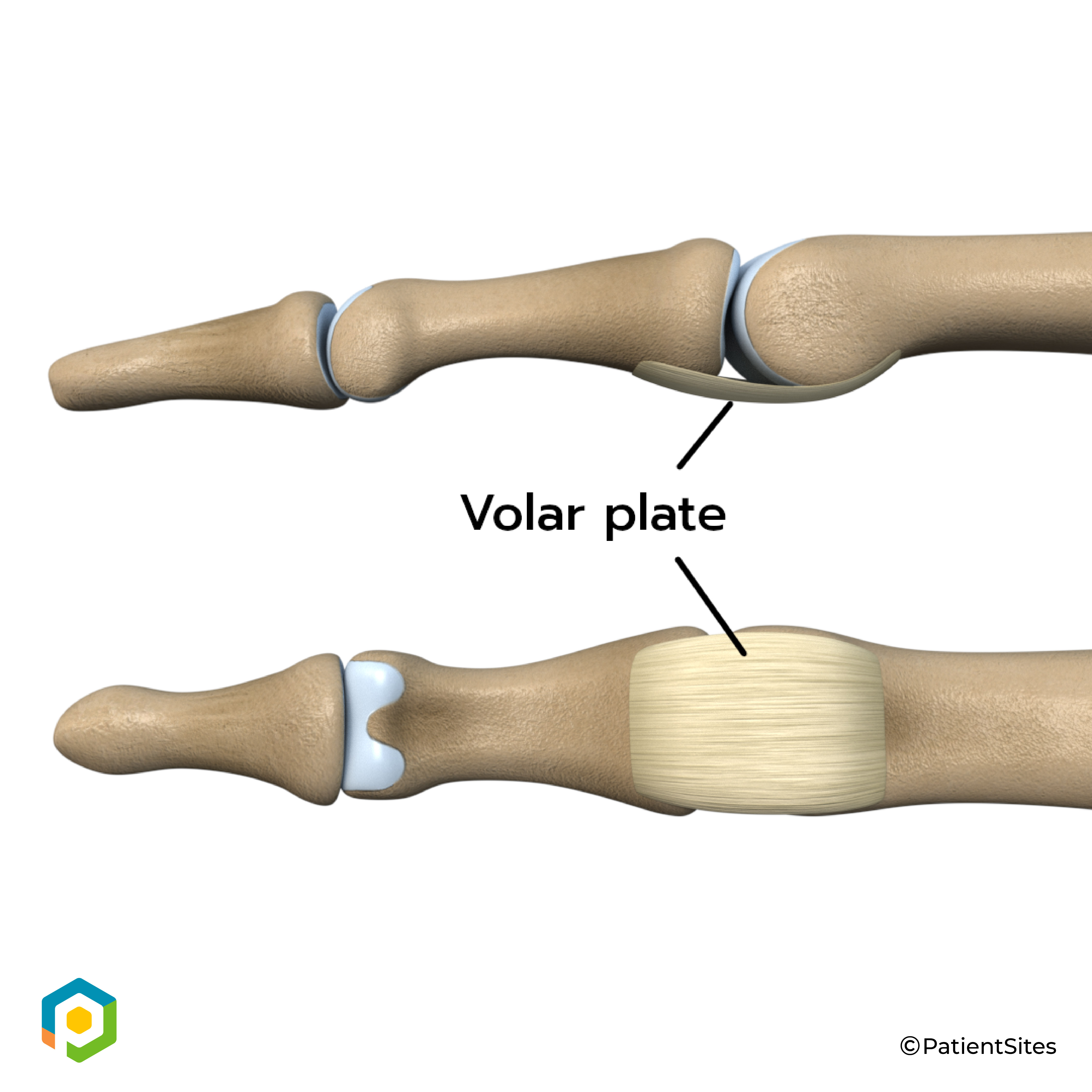
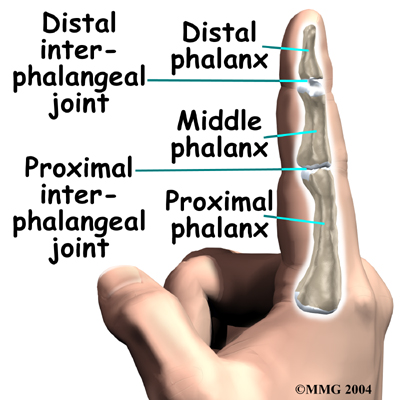 The fingers are actually made up of
The fingers are actually made up of 
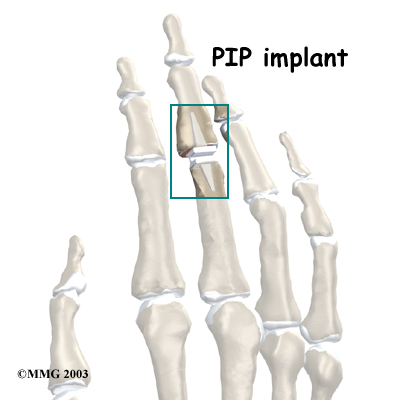 PIP Joint Arthroplasty
PIP Joint Arthroplasty
 (403) 679-7179
(403) 679-7179  concierge@one-wellness.ca
concierge@one-wellness.ca 

