What might go wrong?
As with all major surgical procedures, complications can occur. This document doesn't provide a complete list of the possible complications, but it does highlight some of the most common problems. Some of the most common complications following revision arthroplasty of the knee include:
- anesthesia complications
- thrombophlebitis
- infection
- myositis ossificans
- loosening
- incision complications
Anesthesia Complications
Most surgical procedures require that some type of anesthesia be done before surgery. A very small number of patients have problems with anesthesia. These problems can be reactions to the drugs used, problems related to other medical complications, and problems due to the anesthesia. Be sure to discuss the risks and your concerns with your anesthesiologist.
Thrombophlebitis (Blood Clots)
Thrombophlebitis, sometimes called deep venous thrombosis (DVT), can occur after any operation, but it is more likely to occur following surgery on the hip, pelvis, or knee. DVT occurs when the blood in the large veins of the leg forms blood clots. This may cause the leg to swell and become warm to the touch and painful. If the blood clots in the veins break apart, they can travel to the lung, where they lodge in the capillaries and cut off the blood supply to a portion of the lung. This is called a pulmonary embolism. (Pulmonary means lung, and embolism refers to a fragment of something traveling through the vascular system.) Most surgeons take preventing DVT very seriously. There are many ways to reduce the risk of DVT, but probably the most effective is getting you moving as soon as possible. Two other commonly used preventative measures include:
- pressure stockings to keep the blood in the legs moving
- medications that thin the blood and prevent blood clots from forming
Infection
Infection can be a very serious complication following an artificial joint revision. Some infections may show up very early, even before you leave the hospital. Others may not become apparent for months, or even years, after the operation. Infection can spread into the artificial joint from other infected areas. Your surgeon may want to make sure that you take antibiotics when you have dental work or surgical procedures on your bladder and colon to reduce the risk of spreading germs to the joint.
The risk of infection is higher in revision arthroplasty than in primary joint replacement. In a primary knee replacement, the risk of infection is less than one percent. It goes up to two percent or more in revision cases. These figures are only an estimate and vary between different scientific studies.
Myositis Ossificans
Myositis ossificans is a curious problem that can affect the knee after both a primary knee replacement and a revision knee replacement. The condition occurs when the soft tissue around the knee joint begins to develop calcium deposits. Myositis means inflammation of muscle, and ossificans refers to the formation of bone. This can lead to a situation where new bone actually forms along the sides and top of the knee. This leads to stiffness and a loss of motion in the knee joint. It also causes pain.
Myositis ossificans is more common in people who have a long history of osteoarthritis with multiple bones spurs. Something about the genetic makeup in these people makes them more likely to produce bone tissue. Major reconstruction operations such as a knee revision seem to do more damage to the surrounding tissues than primary knee replacements. The operation is simply longer and harder to do. Calcium deposits are also more likely to form.
The treatment of myositis ossificans may actually begin before you get it. In cases where you are at high risk for developing this condition, your surgeon may recommend that you take medications such as indomethacin after surgery. This medication reduces the tendency for bone to form and may protect you from developing myositis ossificans.
A much more effective method that has been used a great deal to prevent the development of myositis ossificans involves radiation treatments immediately after surgery. These are the same type of radiation treatments used to treat cancer. Several short radiation treatments begun the day after surgery and continued for three to five days seem to drastically reduce the risk of developing myositis ossificans.
If myositis ossificans forms despite these precautions, treatment will depend on how much it affects your knee. Your surgeon will note how much pain it causes and how much it restricts motion. In some severe cases, you may choose to have a second operation to remove the calcified tissue that has formed. This is usually followed by radiation treatments to prevent the calcium deposits from returning.
Loosening
The major reason that artificial joints eventually fail continues to be from loosening where the metal or cement meets the bone. A loose revised prosthesis is a problem because it causes pain. Once the pain becomes unbearable, another revision surgery may be needed. The rate of loosening is higher after revision surgery than in primary arthroplasties.
Incision Complications
Poor healing of the incision is a fairly common complication of knee revision arthoplasty. This is because the tissue is often scarred and thinner than when the original knee replacement was done. The blood supply to the skin may not be normal due to damage to the blood vessels from one or more previous knee surgeries. As mentioned earlier, previous skin incisions can make it hard for the incision to close after knee revision surgery, leading to complications. When the incision doesn't heal right, the chances of infection go up. The wound may continue to ooze, creating optimal conditions for bacterial growth.
Poor incision healing is more likely to occur in patients with one or more of the following factors:
- anemia
- obesity
- past wound healing problems
- weak immune system
- tobacco habit
- poor circulation
- diabetes mellitus
Your surgeon's goal is to prevent problems with the incision. If problems do happen, however, one or more additional surgeries will likely be needed.
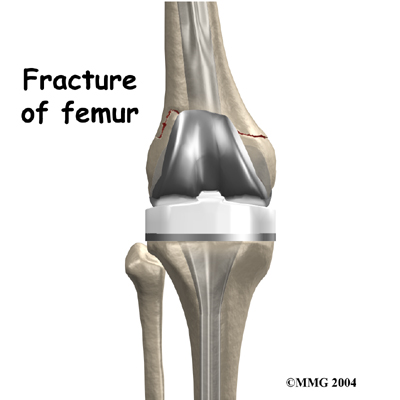 Fracture
Fracture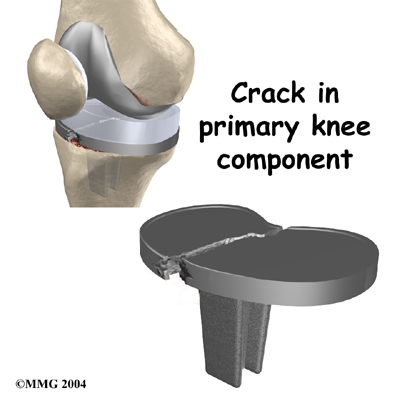
 If your surgeon suspects that the artificial knee is loose, other tests may be necessary to find out why the joint is loose. Before any plans are made to revise the artificial joint, most orthopedic surgeons will want to make sure that the knee is not loose because of infection. To check for infection, blood tests may be ordered. Your surgeon may also need to
If your surgeon suspects that the artificial knee is loose, other tests may be necessary to find out why the joint is loose. Before any plans are made to revise the artificial joint, most orthopedic surgeons will want to make sure that the knee is not loose because of infection. To check for infection, blood tests may be ordered. Your surgeon may also need to 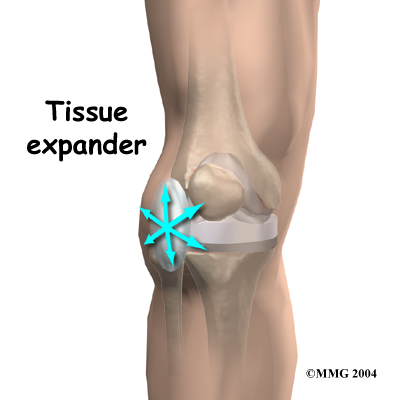 Another option is to use
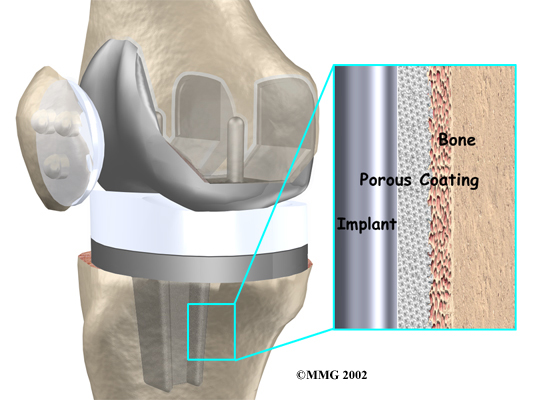
Another option is to use 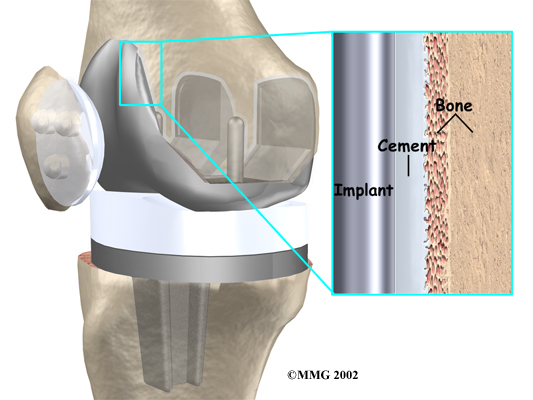
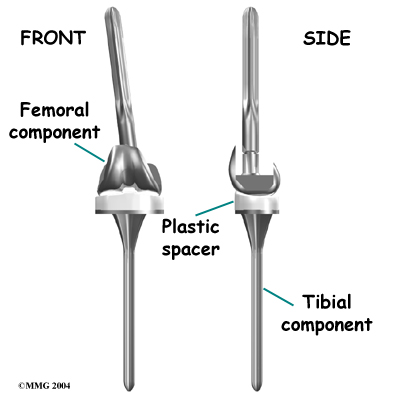
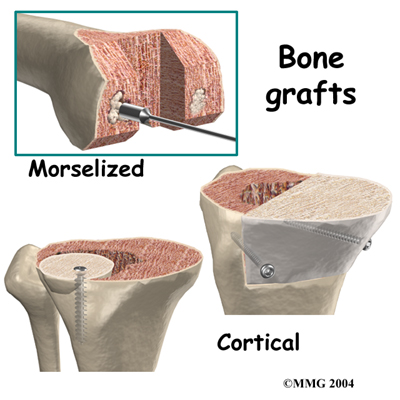 Revision joint replacements are much different from primary joint replacements. One reason that revision procedures are not routine is that there is almost always bone loss around the primary prosthesis. The surgeon deals with this problem by placing a
Revision joint replacements are much different from primary joint replacements. One reason that revision procedures are not routine is that there is almost always bone loss around the primary prosthesis. The surgeon deals with this problem by placing a 
 (403) 679-7179
(403) 679-7179  concierge@one-wellness.ca
concierge@one-wellness.ca 

